
As discussed in introduction section 0.01, we have briefly mentioned the importance of plaque formation and the potential damage it can cause. In this article, we will focus primarily on the infants and children. More importantly, we will have a better understanding on we can positively impact our children’s oral health.
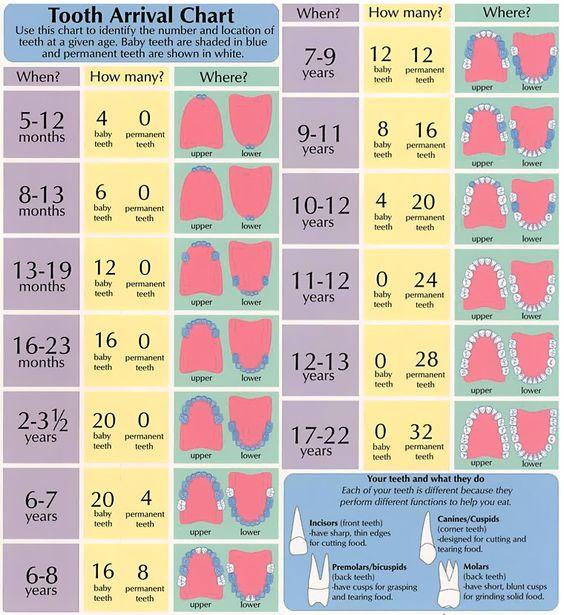
First, let’s look at figure 1 and understand our teeth eruption pattern. Please note that this only an average and should be used for reference, so do not worry if your child is early or late in terms of their teeth eruption. However, it is still wise to have annual x-rays taken to make sure there are no abnormalities or potential problems that may cause complications in the future. As their baby teeth come out, it may be normal if infants show signs such as higher body temperature, diarrhea, increased salivation, dehydration, skin eruptions, and gastrointestinal disturbances1, 2, 3. Under these signs, what may usually help alleviate the symptoms are increasing their fluid consumption, using teething rings that may help apply cold or pressure to the area, or, if necessary, even nonaspirin pain medication. This would help result in happier babies.
One of the most important strains of bacteria in our mouth that cause cavities is Streptococcus mutans. With our carbohydrate intake, it provides food for the bacteria existing in our mouth. Sequentially, acid is produced as by-product and causes tooth cavities. It has been proven long ago that bacteria such as S. mutans and many other strains get transferred to infants through “vertical transmission”, such as mouth-to-mouth transmission between mothers and their children4. That is, direct transmission from sharing saliva (e.g. kissing) as well as indirect transmission from sharing items that go in both parents’ and infants’ mouth (e.g. spoon, food, pacifier, etc.). Therefore, with these findings, oral hygiene and reducing the bacteria in mothers (or whomever the caretaker is, for that matter) is just as important in order to delay or maybe even prevent transmission of bacteria as infants’ primary teeth erupt5, 6. “Horizontal transmission” is also noted and suggested when S. mutans with identical genotypes were found in children from the same nursery school ranging from 12-24 months of age7, 8.
Hopefully this gives us a better understanding of what to expect as infants start their teething process and how we can better plan a prevention regimen to lessen the chance of cavities. Minimizing the transfer of oral bacteria can and will definitely help create a better opportunity for our children to build a healthier mouth. Stay tuned for more useful tips and information!
References
- Barlow BS, Kanellis MJ, Slayton RL: Tooth eruption symptoms: a survey of parents and health professionals. J Dent Child 69:148-150, 2002.
- Macknin ML, Piedmonte M, Jacobs J, et al: Symptoms associated with infant teething. A prospective study. Pediatrics 105:747-752, 2000.
- Wake M, Hesketh K, Lucas J: Teething and tooth eruption in infants: a cohort study. Pediatrics 106:1374-1379, 2000.
- Berkowitz RJ, Turner J, Green P: Maternal salivary levels of Streptococcus mutans and primary oral infection of infants. Arch Oral Biol 26:147, 1981.
- Kohler B, Bratthall D, Krasse B: Preventive measures in mothers influence the establishment of the bacterium Streptococcus mutans in their infants. Arch Oral Biol 28:225, 1983.
- Söderling E, Isokangas P, Pienihäkkinen K et al: Influence of maternal xylitol consumption on mother-child transmission of mutans streptococci: 6-year follow-up. Caries Res 35:173, 2001.
- Mattos-Graner RO, Li Y, Caufield PW et al: Genotypic diversity of mutans streptococci in Brazilian nursery children suggests horizontal transmission. J Clin Microbiol 39:2313, 2001.
- Tedjosasongko U, Koazi K: Initial acquisition and transmission of mutans streptococci in children at day nursery. J Dent Child 69:284, 2002.